Sociodemographic of respondents
A total of 140 households completed surveys with a response rate of 45.0%. The respondents were comprised of 48.6% males (n = 68) and 51.4% females (n = 72) in the general population aged 18 to 64 years, which were differentiated into five age groups: ≤19 (1.4%); 20–29 (22.1%); 30–50 (67.1%); 51–59 (5.0%); ≥60 (4.3%). There was a variation in terms of education levels and employment status; the majority of respondents were Bachelor-degree holders (at least 45%) and working as government servants (60.0%), as tabulated in Table 1. The accounted median monthly household income of Putrajaya is RM 7512 (~USD 1803, mean monthly household income of RM 10401, ~USD 2496), exceeding the national level (RM 4585, ~USD 1100)26. The survey covered household groups: bottom 40% (B40), middle 40% (M40), and top 20% (T20), classified into income groups ≤RM 2999, RM 3000–4999, RM 5000–6999, RM 7000–8999, RM 9000–10999, RM 11000–12999, and ≥RM 13000, where RM 1 approximately equivalent to USD 0.24 in average. On an average, respondents had lived in Putrajaya for seven years.
Table 1 Descriptive statistics about risk perception of drinking water supply security with potential EDC contamination.
Human morphology and drinking water consumption patterns
The present study involved 140 households with 257 total respondents (n = 257), consisting of infants (n = 4, aged less than 1 year; birth–5; 6–11 months), children (n = 77, aged 1 to 9 years; 1–3; 4–6; 7–9 years), adolescents (n = 37, aged 10 to 19 years; 10–14; 15–19 years), adults (n = 133, aged 20 to 59 years; 20–29; 30–50; 51–59 years) and elderly (n = 6, aged more than 60 years) (Table 2). Age groups were categorized based on previous studies27,28,29,30.
Table 2 Age groups and respective mean body weight, body height, body mass index, daily water intake, and daily water intake per body weight.
There were no significant differences between males (n = 125) and females (n = 132) in terms of body weight (t(235) = 1.671, p = 0.096), body height (t(225) = 0.804, p = 0.422), body mass index (t(246) = 1.116, p = 0.266), and daily water intake (t(255) = 0.483, p = 0.629). Surprisingly, males consumed more water than females in the United States and Australia19,31. Body weight showed a significant positive correlation to height based on Pearson product-moment correlation test (r = 0.861, p < 0.001). Moreover, daily water intake was observed positively correlated to body weight (r = 0.376, p < 0.001) and height (r = 0.347, p < 0.001), indicating the potential influence of human morphology and growth in daily water consumption. Table 2 depicts the mean body weight, body height, body mass index, daily water intake, and daily water intake per body weight of the respective age group in the present study. Age groups had a significant difference in term of body weight, body height, body mass index, and daily water intake (one-way analysis of variance, p < 0.001). Malaysian frequency of exposure to pollutants in tap water was 1 (365 days/365 days, 95th-percentile value).
Drinking water ingestion pattern varied between life stages (Fig. 1). The difference was due to the changes in human behavioral and physiological characteristics (development and age-specific) under varying environmental conditions19. The early life stage (infants and children) had greater drinking water ingestion on a body weight basis compared to adolescence and adulthood. Further, Fig. 1 depicts the comparison of daily water intake per body weight in the present study to US EPA19 guidelines for exposure assessment. American adolescents consumed drinking water at the lowest rate; meanwhile, the present study reported the elderly (≥60 years of age) to have the lowest water intake rate. Both studies revealed the constant daily drinking water intake per body weight throughout adulthood. The lower daily water intake rate of elderly Malaysians was related to the younger retirement age and thus the lower energy consumption and water restoration. Thus, the application of regional data for exposure and health risk assessment may be less relevant in some regions because of the variation in contamination, human growth, and drinking water intake across the world. The limitation of not having detailed particulars on drinking water intake and body weight of the local population was highlighted in a previous study18. Therefore, data collection and analysis on the local human morphology, drinking water consumption patterns, and household practices regarding tap water as drinking water were done to better reflect local exposures to EDCs.
Fig. 1: Comparison of consumers’ daily water intake per body weight in the present study to US EPA guideline.
Human growth and drinking water intake vary. The variation concerns the relevance of the application of regional data for exposure and health risk assessment. Data from US EPA guidelines are based on ref. 19.
Household practices on tap water as drinking water
A majority of households (52.9%) were observed taking both bottled and tap water as their daily drinking water sources. The remainder chose either only tap water (35.7%) or bottled water (11.4%). A high percentage of households (87.1%, n = 122) practice tap water treatment before daily consumption as drinking water (Fig. 2a). Other households (n = 18) do not treat water as drinking water as most of them (16 out of 18 households) were consuming only bottled water, whereas only two of them had a direct intake of tap water without any treatment. Comparatively, bottled water was primarily chosen among consumers in other countries such as the United States, Australia, Canada, Czech Republic, France, Italy, Korea, Mexico, the Netherlands, Norway, and Sweden32,33.
Fig. 2: Household practices for using tap water as drinking water for adults and children.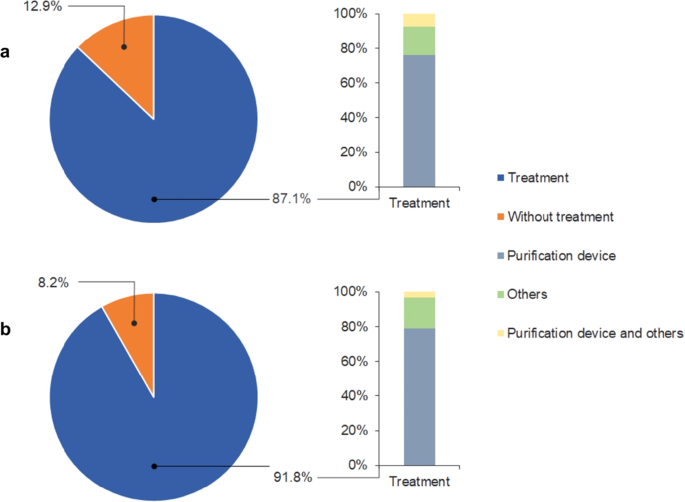
Majority of households purified tap water before daily consumption as drinking water. a Adults. b Children.
There were a higher proportion of males in the profiles of (i) both bottled and tap water (54.4 and 51.4% of males and females, respectively) and (ii) individual tap water (36.8 and 34.7% of males and females, respectively), but not that of individual bottled water (8.8 and 13.9% of males and females, respectively). The least selected option, consumption of bottled water, was only slightly more preferable by females compared to males (5.1% difference). Choice of tap water only was more favorable among houseworkers and retired people who stay at home for longer than those who chose otherwise; thus, it was the elderly (aged ≥60 years) with the highest proportion at 66.7% (the remaining 33.3% preferred tap water mix with bottled water). Up to 83.3% of T20 consumers (household income ≥RM 13000) were prone to drink tap water only (in contrast, the other 16.7% chose bottled water only), whereas B40 and M40 consumers (household income ≤RM 12999) preferred to mix the use of bottled and tap water (47.6–60.0%), followed by tap water only (27.3–47.6%). People with postgraduate qualification (Masters and Doctorate) prioritized the option of tap water only at a proportion of 48.1 and 66.7%, respectively, which was higher than the other education levels (ranged between 22.9–38.1% versus 50.0–68.6% for the combination of bottled and tap water). The association between demographic characteristics and household choices of drinking water was similar to the previous study, except that a higher proportion of males were recorded as choosing bottled water only5.
Based on the survey, attachment of home purification systems, i.e., point of use (connected directly to the tap) and point of entry (connected where the water enters the house) were common among the households. As shown in Fig. 2a, treatment with a purification device was the most practical treatment method (76.2%). Some households tended to further boil the purified tap water for their daily drinking water consumption (7.4%). Meanwhile, 16.4% responded that boiling was their only treatment practice. A chi-square test found no significant association between demographic characteristics and household choices about drinking water (p > 0.05); that is, households of different demographic groups made choices about daily drinking water sources and treatment which were independent of their group categorization. Surprisingly, age and gender were the significant variables in choosing bottled water as the source for drinking water32.
Among the respondents, 67.9% were married (n = 95, only 73 of whom had children), followed by those who were never married (31.4%, n = 44) or divorced (0.7%, n = 1). All parents had the same drinking water sources and practices regarding tap water as for their children’s daily water intake. Over half of the parents (52.1%) provided their children with bottled and tap water in combination, followed by tap water (39.7%) or bottled water (8.2%) only. Filtration using a purification device was the most preferred practice (79.1%) before allowing children to drink water, followed by boiling (17.9%) and employment of both filtration and boiling (3.0%), except for those consuming only bottled water with no household treatment (Fig. 2b). Moreover, there was an association between the age group of parents and their practices preparing tap water for their children to drink (χ2(6) = 13.24, p = 0.039). Parents aged 20–29 years choose equally between filtration and boiling method. A higher proportion of respondents in age groups 30–50 and 51–59 (at least 80.0% among them) preferred filtration using a purification device. Nonetheless, up to 33.3% of parents in the age group ≥60 years chose a combination of filtration and boiling, although filtration was the preferred method (66.7% among them).
Households were taking both bottled and tap water at the same time, and resorted to bottled water when they lost trust in tap water quality for drinking7,32,33. Also, households were most likely to purchase bottled water and use home purification systems; this is attributed to the households’ perception of the better quality, safety, taste, health characteristics, and naturality (mineral water), with affordability, convenience, and social values7,8,32,33,34,35. However, these perceptions and claims were debatable in terms of the actual quality and long term effects of exposure on a regular basis. For example, the dominant presence of contaminants such as mineral ions (e.g., sodium, potassium, calcium, and magnesium) and EDCs (e.g., plasticizers) in bottled water (mineral and drinking water) with relatively low physicochemical parameters of the drinking bottled water36,37. Moreover, the efficiency of purification devices is of great concern when the diverse organophosphate flame retardant contamination and exposure have been attributed to water purifiers16. Meanwhile, the households’ choice of using tap water as the main daily drinking water source in the present study raises concerns for human exposure to EDCs through daily consumption of drinking water since treatment systems (both treatment plants and home devices) have been proven to be inefficient in removing these emerging contaminants.
Actual risk of EDCs in drinking water
Given that EDCs are present in tap water, a primary choice of drinking water supply among the consumers, humans are potentially exposed to EDCs via drinking water intake. Therefore, regional database profiling is useful to better reflect local exposure and health risk. This involves further incorporating collected data into human health risk assessment with monitoring data, as shown in the following equations. The estimation of human life-stage health risks with varying local age-specific exposure was able to reduce uncertainty in the exposure assessment and provide a more conservative worst-case scenario. A risk quotient (RQ) value greater than 1 indicates a possible risk of exposure through drinking water.
$${{{mathrm{RQ}}}} = {{{mathrm{C}}}}_{{{mathrm{s}}}}/{{{mathrm{DWEL}}}}$$
(1)
$${{{mathrm{DWEL}}}} = left( {{{{mathrm{ADI}}}} times {{{mathrm{BW}}}} times {{{mathrm{HQ}}}}} right)/left( {{{{mathrm{DWI}}}} times {{{mathrm{AB}}}} times {{{mathrm{FOE}}}}} right)$$
(2)
where Cs is the maximum detected concentration (ng/L, to be obtained from monitoring work); DWEL is drinking water equivalent level; ADI is the acceptable daily intake (ng/kg/day); BW is body weight (kg); HQ is the hazard quotient; DWI is the drinking water intake (L/day); AB is the gastrointestinal absorption rate; and FOE is the frequency of exposure (days/365 days)38,39. Table 3 shows the exposure factor definitions and values used in human health risk assessment.
Table 3 Exposure factor definitions and values used in human health risk assessment.
Residues were categorized into four groups: (a) residues with all life-stage RQs > 2.5 × 10−3, (b) residues with all life-stage RQs between 2.5 × 10−4 and 2.5 × 10−3, (c) residues with at least one life-stage RQ between 2.5 × 10−5 and 2.5 × 10−4, and (d) residues with all life-stage RQs < 2.5 × 10−5. Lifetime RQ profiles from birth to 60 years of age in relation to daily water intake per body weight are depicted in Fig. 3. The estimated RQs of the nine EDC residues via drinking water were ≤1.30 × 10−2, with the highest at age ≤5 months under dexamethasone exposure. RQs in early life stages, i.e., infants and children (birth to 9 years) were higher than the RQs of adolescents (at least 1.6–3.2 times), adults (at least 2.0–3.4 times), and elderly (at least 2.7–4.4 times), respectively. Among the life stages, infants (birth to 5 months) possessed the highest health risks, whereas the elderly (≥60 years) exhibited the lowest health risks. The potential exposure levels and human health risks were constant throughout adulthood. Human health life-stage RQ profile was highly dependent on the daily water intake per body weight (Fig. 3). RQ of the EDC mixture was estimated based on the summation of individual RQ values of each EDC, accounted highest at 3.28 × 10−2.
Fig. 3: Human health life-stage RQ profile of detected mixture and individual EDC residues in tap water in relation to daily water intake per body weight.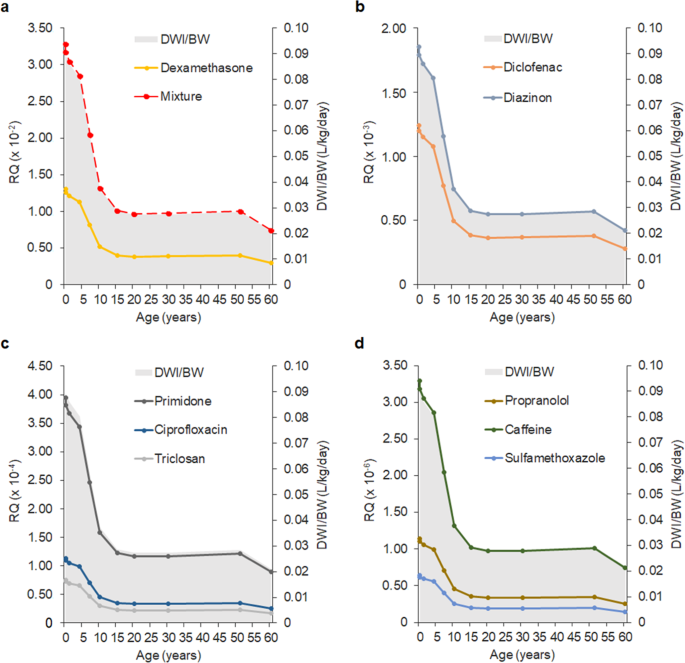
There was no potential risk of EDC exposure to all the life stages via drinking water intake (RQ < 1) in the present study. a EDC mixture and residue with all life-stage RQs > 2.5 × 10−3. b Residues with all life-stage RQs between 2.5 × 10−4 and 2.5 × 10−3. c Residues with at least one life-stage RQ between 2.0 × 10−5 and 2.5 × 10−4. d Residues with all life-stage RQs < 2.5 × 10−5. DWI/BW Daily water intake per body weight, RQ Risk quotient.
RQ values less than one estimated that there were no potential risks to all the life stages under present exposure to individual and mixture EDCs via drinking water consumption. However, increasing application and unregulated discharges of EDCs based on the (i) inadequate evidence (epidemiological studies) about the risk of human exposure, (ii) underdeveloped risk communication and governance (regulation and public participation), and (iii) unknown risk perception and its role in adopting risk prevention and intervention, will further increase contamination and human exposure9. Nevertheless, the present study presented a questionnaire survey in regional database profiling, which is supportive in human health risk assessment of reducing the environmental pollution of EDCs and managing human exposure to them through drinking water ingestion.
Perceived risk of drinking water supply quality
Mean perception of risk, at 2.42 ± 0.71, was between the points “unsure” and “agree” to the issue of present drinking water supply security with the potential of EDC contamination. The public perceived every water quality and health issue as significantly different (F(3, 556) = 38.844, p < 0.001). Notably, up to 85% of the population was highly concerned about tap water quality (2.81 ± 0.50); however, the concern was less likely attributed specifically to the presence of EDCs (2.57 ± 0.64) (p = 0.013). The public was relatively unsure whether tap water was safe to drink (2.02 ± 0.78), as well as the capability of the Malaysia Drinking Water Quality Standard to regulate EDCs in tap water (2.29 ± 0.70). Approximately 39.3% perceived that the Malaysia Drinking Water Quality Standard was capable of regulating EDCs in tap water, although most of the EDCs were not currently regulated under the guideline.
The influence of sociodemographic group on actual or perceived proximity to a potential risk was observed with the affected risk perception of drinking water quality (amplification or attenuation effects)6,25,40. Table 1 shows a breakdown of the mean score of public risk perception of drinking water supply security with the potential EDCs contamination and the statistical difference for each of the sociodemographic variables. Overall, a significant difference was observed only in gender, where males (2.49 ± 0.66) perceived a higher risk than females (2.35 ± 0.75) (t(555) = 2.321, p = 0.021). In this context, males were more confident that Malaysian tap water was safe to drink (2.24 ± 0.74) and the Malaysia Drinking Water Quality Standard was capable of regulating EDCs in tap water (2.44 ± 0.58) than females (1.82 ± 0.78 and 2.14 ± 0.68, respectively). An independent-samples t-test showed that the differences between the genders were significant (t(138) = 3.253, p = 0.001 and t(138) = 2.822, p = 0.005, respectively).
To illustrate the differences between individuals who had a high or low perception of risk of EDCs in tap water, they were classified into different risk perception communities as follows: low risk perception (i.e., scored ≤2.00 on average; this constituted 27.1% of the respondents) and high risk perception (i.e., scored ≥2.75 on average; this constituted 35.7% of the respondents). Figure 4 depicts a comparison of mean responses of the low- and high-risk perception communities about drinking water supply quality. The low- (1.87 ± 0.74) and high-risk perception communities (2.90 ± 0.30) perceived risk concerning drinking water supply significantly differently at t(188) = −16.141, p < 0.001.
Fig. 4: Comparison of mean responses between low- and high-risk perception communities about drinking water supply quality.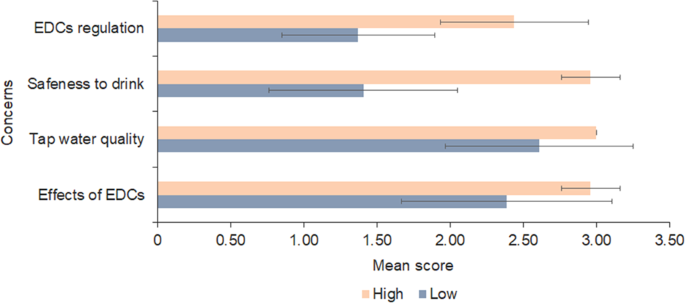
Error bars represent standard deviation.
Most of the males (45.6%) perceived high risk regarding the daily supply of drinking water; meanwhile, there was a higher proportion of low-risk perception females (2.8% higher than the high-risk perception females). Figure 5 shows the proportion of each risk perception community within different groups of demographic characteristics. The high-risk perception community was mostly comprised of the working groups such as government servants, private workers, and self-employed individuals, as well as the retired workers. Similarly, the elderly (aged ≥60 years) had a higher risk perception than the other younger respondents (Fig. 5 and Table 1). Different education levels made up the greater proportion of the high-risk perception community, in which field of study could be an underlying factor. Wealthy people had different risk perception to lower income people; notably, the high-risk perception community had no T20 income group. Also, up to 60% of the M40 income group were in the high-risk perception community. Moreover, the B40 income group had relatively high risk perception (30.3 and 24.2% of high- and low-risk perception groups, respectively). Nonetheless, the chi-square test found no significant influence of demographic characteristics in the distribution of risk perception communities (p > 0.05). Beside the sociodemographic factors, the variation in public-perceived risk of EDCs in drinking water was expected due to the different risk processing either based on a rational system (analytical processing system) or a nonrational system (experiential processing system)9. Further, future studies on comprehensive conceptualization of the risk processing system and predictors (e.g., cognitive and affective) are required for in-depth analysis of the public responses to the risk perceived in the emerging drinking water quality issue.
Fig. 5: Proportion of low- and high-risk perception community within different groups of demographic characteristics.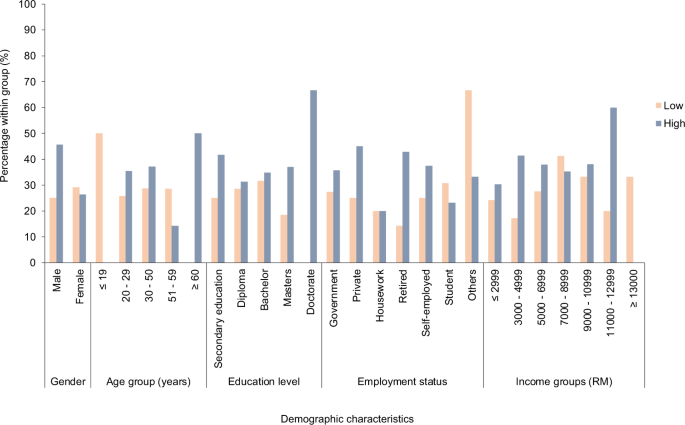
The chi-square test found no significant influence of demographic characteristics in the distribution of risk perception communities (p > 0.05), whereby the risk processing system could be the influencing factor.
The present study observed the current risk perception level with the presence of a low-risk perception community and a group of people who were unsure of the emerging drinking water quality issue. The situation indicates the lack of effective communication and governance in developing countries since the broad scope of EDCs had been widely detected in global drinking water supply, particularly pharmaceuticals in Malaysian tap water39. Further, it is not a worldwide practice to raise awareness and regulate emerging contaminants in drinking water. Subsequently, development of risk behavior (preparedness, reduction, prevention, and mitigation) and adoption of public participation in a multi-barrier approach in the monitoring and management framework of the drinking water supply system are challenging. Thus, the present study, which contributes empirical and theoretical outputs, facilitates the conceptualization of effective communication and governance, targeting the dissemination of information on safe drinking water quality and public involvement in regard to EDCs. This supports the national water sector in accomplishing the Sustainable Development Goals (SDGs) that target clean drinking water and sanitation, and safeguard public health for all.
[ad_2]
Originally Appeared Here